

Overview
Arthritis is an extremely common condition that develops in the knee over time most often due to wear and tear on the knee joint. Arthritis results in a loss of articular cartilage, the gliding surface of the knee. This results in a progressive roughening of the surfaces within the knee. Pain and swelling results, especially with increased activity.
Certain patients develop arthritis due to malalignment of the knee. Malalignment means that the weight of the body is distributed unevenly across the two knee compartments. Most malalignment in knees is due to excessive varus alignment (bow-legged) causing narrowing of the joint space on the inner (medial) aspect of the knee. Occasionally, a knee has too much valgus (knock-kneed) causing narrowing of the outer (lateral) aspect of the knee.
There are many mild cases of arthritis and malalignment that can be managed with conservative measures. These conservative measures include, rest, icing, NSAIDs (anti-inflammatories), physical therapy, bracing, assistive devices, and activity modification. When these measures fail to control pain and the patient is unsatisfied with the quality of life allowed by the knee, surgery can be an effective treatment for the pain associate with arthritis.
The three surgical treatments available for arthritis in the medial compartment are high tibial osteotomy, unicompartmental knee replacement, and total knee replacement. Because knee replacements fail over time, in younger patients (age 35-55) it is often preferable to salvage the knee joint rather than directly proceeding with a knee replacement. In addition, a patient that would like to return to impact activities and/or labor would likely be limited by a total knee replacement whereas a knee after osteotomy can tolerate these higher demand activities without the risk of loosening or failure that is inherent with knee replacement. The following case example demonstrates a patient with varus malalignment and knee arthritis that underwent a high tibial osteotomy (Figure 1).
Figure 1. The diagram below is an exaggerated depiction of varus malalignment of the knee. The straight line represents the weight bearing axis of the leg as measured from hip to ankle. With malalignment and varus deformity, this axis falls through the painful medial (inner) compartment. The surgery involves cutting the tibia bone to realign the knee so weight is borne the normal preserved cartilage of the lateral (outer) compartment. A specially designed plate and screws holds the bone in the new position while it heals. Long term results have shown that most patients obtain ten years of pain relief and improved knee function from the osteotomy. A knee replacement can still be performed in the future if necessary.
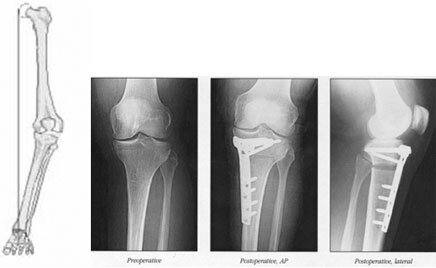
Figure 1
Surgery
- General or epidural anesthesia is required.
- Preoperative templating plans exactly the amount of correction needed using full length, standing x-rays.
- A four-inch incision centered over the tibia is made.
- Surgical time is two hours to perform the osteotomy and apply the plate and screws.
- Hospital stay averages 2 days
- No weight bearing is allowed for six weeks while the bone heals. During this time, the patient is strictly on crutches.
- A continuous passive motion machine (CPM) will be used for 2-4 weeks to restore range of motion of the knee.
- Icing 20-30 minutes 3-4 times per day helps reduce swelling.
- The incision is kept dry for 7-10 days.
- X-rays and a follow-up visit are taken at 2, 6, and 12 weeks after surgery to document healing of the osteotomy site and to check range of motion.
- You may need between 2-12 weeks off from work depending on the physical requirements of your job.
Am I a Candidate for High Tibial Osteotomy?
If a patient has isolated arthritis in the medial compartment, is young, and has tried all conservative measures to control pain, a high tibial osteotomy may be an effective option to relieve pain, improve function, and delay knee replacement. Patients greater than 60 and patients with arthritis in multiple knee compartments are better served with total knee replacement.
Distal Femoral Valgus Osteotomy
Occasionally, a patient has progressive pain due to excessive valgus deformity (knock kneed) and requires an osteotomy in the opposite direction (to create increased weight bearing in the medial compartment). In this setting, the osteotomy is still performed at the knee, but on the femoral (thigh bone) side of the knee. Surgical details are similar. Figure 2 shows a knee that was corrected for excessive valgus (knock-kneed).

Figure 2. A distal femoral osteotomy has been performed on the left knee to correct excessive valgus deformity.



